


After Getting COVID, Part 1


{kind=link}
At last we get to the leading edge of what I promised for my friend. He and his partner have differing flavors of Long COVID. They don’t know what they can do about it.
Disclaimer: Everything in this After Getting COVID series of posts is YMMV (Your Mileage May Vary). I’m not a doctor. I can tell you what I have experienced, read, heard, etc. but I cannot promise what it will do for you. I also don’t know your personal health history, what you already take or what you already do. If you have contraindications, I’m not the right person to recognize that and tell you. Your pharmacist and/or doctor can help you check for those before you try something.
For clarity, SARS-CoV-2 (SARS2 for short) is the cause of a disease called COVID, similar to the way HIV is the cause of a disease called AIDS.
It would be misleading for me to say this is only about Long COVID (prolonged symptomatic illness in the wake of an acute infection). As research peels more layers of the onion toward what SARS2 does, it is more and more clear that after a person has an infection with SARS2, there are usually (maybe always) long term consequences. What distinguishes Long COVID patients is that their long term consequences are obviously post-acute and too big to ignore, and their symptoms carry on a long time, perhaps years. Many people who first got COVID in early 2020 are still sick with no recovery in sight.
Please use the links embedded in this post as a starting point to learn more about specific items.
What Does SARS-CoV-2 Do?
As I have mentioned before, the virus is misnamed. Severe Acute Respiratory Syndrome, SARS. Severe? Yes. Respiratory? Not necessarily.
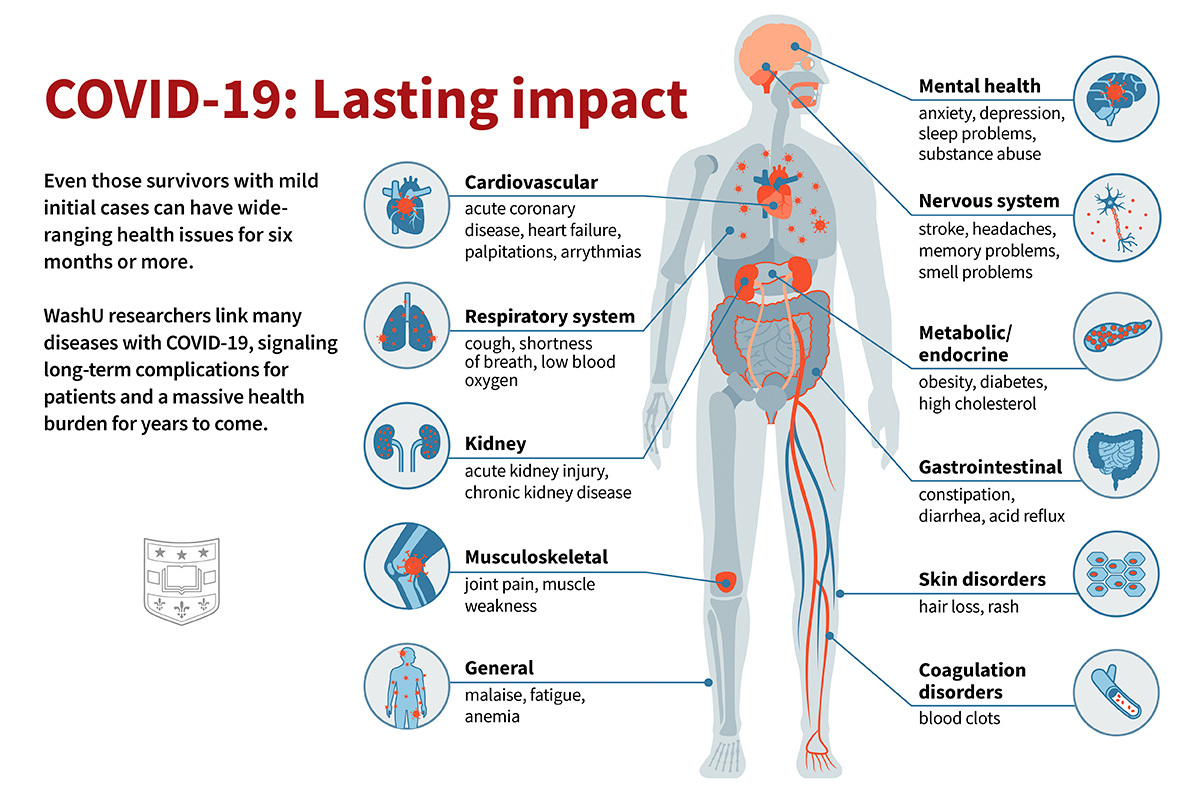
SARS2 can get into many of our tissues and organ systems. It can wreak havoc anywhere it chooses.
As the picture began to unfold, I especially noticed damage in the brain as documented early on in the UK biobank brain scan study. But it is highly fond of the endothelium, a layer of cells that line blood vessels and lymphatic vessels. It is also fond of the heart, immune system, digestive tract, liver, kidneys… and yes, lungs… among other systems. Within cells, it shortens telomeres (associated with aging) and disrupts mitochondria (the “power plants” inside cells). You see what I mean about how broad its scope is.
So far, science hypothesizes that SARS2 doesn’t persist in everyone who gets COVID. If that is true, it’s “better” than HIV where the virus can’t be eliminated after a person gets infected. But we aren’t certain it’s true.
SARS2 leaves lingering damage even when a person didn’t have symptoms when they got infected. It isn’t clear yet how long it takes for people to mend that damage if they do kick out the virus and avoid catching it again. We don’t want to think the damage is permanent. Some of it could be, no matter what we want to think.
If you don’t understand how a hit-and-run infection could leave permanent damage, polio is an example. Post-polio syndrome shows us how a person can get better after a hit-and-run virus, then gradually slide much later. If you’re curious about it, I wrote about it for the Forum long ago and kept a copy on my personal website.
For my friend’s purposes, we have to work with what we’ve got so far. We have research findings and a methodology for how to grapple with a Dratted Disease. Post-COVID problems are a DD.
After catching SARS2, people can be left with Long COVID. (More than 200 symptoms are associated with LC. Nobody gets them all at once.) Even if they aren’t aware of being less well than they used to be, they are more vulnerable to getting sicker from anything else they catch, and their risk is elevated for a wide range of health problems including but not limited to heart attack, stroke, blood clots and microclots, kidney disease, gastrointestinal trouble (including severe appendicitis), brain injury, dementia… It’s a long list.
If you want to know more, What SARS-CoV-2 Does to the Body includes some good graphics to show you what the virus does to the human body and it relates to findings from over 100 studies. If the introductory text sounds frustrated… I think we can understand why.
Your Mileage May Vary
With many DDs, each possible treatment or strategy comes with the caution Your Mileage May Vary (YMMV). What helps someone else might not do well for you. What helps you might not do well for someone else.
That applies heavily after you’ve had COVID. I have not seen anything turn up that consistently helps every patient who tries it. Use your methodology for trying out ideas!
Rest, Rest, Rest
In many ways Long COVID patients know more than the scientific and medical community about living with this DD, so I listen to them and I recommend that you do, too. Their advice meshes well with what I learned in the Chronic Illness Forum about diseases that overlap with Long COVID.
Long COVID patients strongly recommend that you rest as much as possible for at least two months after a bout with COVID. Many of them go on to recommend that you avoid heavy exertion for at least a year after acute COVID. Many say this is what they didn’t do and they are certain it contributed to either developing Long COVID or worsening it.
If you develop Long COVID, aggressive rest is not optional. It is necessary. The more you push yourself, the more likely you are to get worse and maybe never get back to where you are now.
Some doctors promote Graded Exercise Therapy (GET) and/or Cognitive Behavior Therapy (CBT) as a treatment for Long COVID, after having done the same to myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) patients for decades.
Do not under any circumstances try GET or CBT.
Formal guidelines say not to do it. Multiple studies prove that GET/CBT can turn a patient with moderately diminished capabilities into someone housebound or bedbound for the rest of their lives.
A subset of Long COVID patients can very gently take up some exercise. This subset are typically people who do not have postural orthostatic tachycardia syndrome (POTS—there is a simple 10 minutes make-do test for it which is good enough and won’t trash you anywhere near as much as a full fledged tilt table test) or post-exertional malaise (PEM). If you are in that subset and choose to try slowly beginning exercise, always stop short of what you feel like you can do. Don’t push yourself.
Use Spoons Wisely
In the Chronic Illness Forum, we described energy in terms of marbles. The energy you have available for the day was a bowl of marbles, and everything you did took marbles out of your bowl. When you ran out of marbles, you couldn’t do anything else.
Our terminology didn’t catch on, but a systemic lupus patient’s explanation of the same concept using spoons at a restaurant table spread like wildfire.
Spoon theory is now a well recognized term among people dealing with chronic illness. If you say you don’t have enough spoons to do something, many people will understand exactly what you mean.
From the Forum, add the 50% Rule to help you manage with the number of spoons (amount of energy) you have. Each day, estimate how many spoons you have available. On your bad days, you don’t have many. On better days, you have more.
As a general practice, don’t even try to use more than half of the spoons you believe you have.
Why? Because contrary to the stories routinely pumped into media about supposedly lazy disabled people, in the Forum we found the opposite. People too unwell to do as much as they want tend to be overly optimistic about how much they can do. They tend to estimate that they have more spoons than they actually have, so they set out to do more than they can really do.
They run out of spoons far short of what they hoped to do in the day. If they try to do more, they overdo it and make themselves more ill. It’s immensely discouraging.
The 50% Rule compensated for excessive optimism. It set goals for the day at a level people could usually reach without wrecking themselves. People still overdid it sometimes, but not as often and not as badly.
What Else Seems to Help At Least Some People
This section will become outdated quickly. Regard it as only a starting point for collecting ideas. Many of these do not have rock solid studies behind them. This is still an emergent disease. In some instances, people have experimented based on their own best guess and found something that a significant number of people tried too, with beneficial effects. Science hasn’t caught up with all of these yet.
Avoiding or Diminishing Another Bout with COVID
If you have Long COVID, getting COVID again can be a disaster. The most effective ways to avoid or diminish another infection with SARS2 are not pharmaceuticals. They include ventilation, air filtration, face masks, specific nasal sprays, etc. Vaccines can reduce your risk of getting severely sick with it, but can’t give you a good shield against infection.
However, it turns out that some drugs can reduce your chance of getting a SARS2 infection that is strong enough to put you in ICU and maybe even diminish your symptoms. It isn’t entirely clear whether they can prevent some infections from happening at all, but they might.
Paxlovid™ is a preferred first-line treatment for acute COVID in the West. It’s still reasonably effective for reducing the chance of having COVID put you on a ventilator. Availability is patchy. In some places cost is a barrier. In other places it is simply not available. Its list of contraindications and possible side effects is long. The metallic taste it may give you goes away after treatment. A standard course of treatment is 5 days even though the manufacturer recommends 10 days. Many patients have a rebound of symptoms soon after finishing a 5 day course.
Metformin is a drug for managing high blood sugar levels in people who have Type 2 diabetes. Used off-label in a 14 day course of treatment, it is one of the next most effective drugs after Paxlovid to prevent acute COVID from becoming severe. It has a much shorter list of contraindications and side effects.
Berberine has emerged as having effects similar to metformin, although it is not as strong. If you can’t get or can’t take metformin, you may be able to take this over-the-counter supplement.
Tenofovir disoproxil fumarate (TDF) is the older formulation of tenofovir. This is an AIDS drug. It helps protect against having COVID become severe. The effect is strongest in people aged 50+.
Protease inhibitors are taken by many HIV positive patients to manage that virus. One study found that people on such drugs had a 70% lower chance of getting symptomatic COVID.
Watch what China is using. The West uses an AIDS drug as one of the components of Paxlovid. China is reportedly making broader use of AIDS drugs against SARS2. Other countries that appear to have some COVID treatments which may be a step up from Paxlovid include Japan (ensitrelvir, marketed as Xocova®, which acts as a protease inhibitor) and Cuba.
Note that some Long COVID patients have gotten some improvement in their baseline condition from treatment with such drugs. Applying these drugs to treat LC rather than in the initial acute phase is off-label use.
Viral Persistence
If you suspect SARS2 has set up camp in your body and isn’t being cleared away (viral persistence), the biggest gain you could get would be from knocking down SARS2 in your body, ideally getting rid of it completely. Nobody has a magic potion to do it, but some things have helped some people (and a few even have proper studies to back them up).
COVID vaccination or booster vaccination. This is a roll of the dice. Sometimes Long COVID improves after it, which suggests the jab helped knock out persisting virus. Sometimes Long COVID gets worse after it, perhaps a challenge the immune system is too exhausted to handle. Sometimes it has hardly any effect on symptoms. There’s no way of knowing in advance which way it will go for you.
Nattokinase is derived from a fermented Japanese food called nattō. In the lab, it attacks and degrades the SARS2 spike protein, so it damages the virus’ ability to infect your cells. I haven’t yet seen studies affirming that it does the same in people. Take it on an empty stomach half an hour before eating.
Serrapeptase is a proteolytic enzyme with anti-inflammatory effects. It also helps break down the clots and microclots that practically every COVID patient develops and that bedevil many Long COVID patients. It is commonly used in Europe and Japan to reduce inflammation and pain after surgery. It is not a good idea to take it if you are already on something that “thins the blood” and extends clotting time. That warning isn’t limited to medications. It also applies to supplements such as turmeric. I have not seen studies to affirm that it helps COVID or Long COVID patients. However, a significant number of Long COVID patients say taking nattokinase and serrapeptase together led to noticeable improvement in their symptoms. Take it on an empty stomach half an hour before eating (with nattokinase if you are taking both).
Streptococcus salivarius K12 (often marketed as BLIS K12) is a bacteria we generally acquire as part of our digestive tract biome when we are babies. Taking it as a probiotic can reduce the severity of acute COVID and can help combat Long COVID. (The gut is often where SARS2 settles in, causing GI problems and probably contributing to a surge in appendicitis cases.) Pay attention to all the parts of that name. I don't see clinical evidence for Streptococcus salivarius M18 (but I haven’t had much time to look yet). BLIS K12 is sometimes packaged with lactose. If you are lactose intolerant, look for a dairy-free formulation. A quick look did not find that easily in the UK, but did find it in the USA.
Vivomixx appears to be more effective as a probiotic against SARS2 in the gut than BLIS K12, but it tends to cost more. You could learn more about probiotics against SARS2 and then keep an eye on new studies to see whether something highly effective but lower cost turns up as an option.
Nicotinamide mononucleotide (NMN) to boost nicotinamide adenine dinucleotide (NAD+). At this point we’re starting to reach toward the more speculative end of what can be done. Research indicates SARS2 heavily draws down the body’s stock of NAD+, which is vital to both metabolism within cells and the immune response to viral infection. Boosting NAD+ should help the immune system fight SARS2. Unfortunately, you can’t directly take NAD+ as a supplement. I looked at the biochemical pathway for it (that link is for a simplified diagram) and chose NMN as what looks like the easiest and most direct supplement you can take to boost a precursor, thereby (in theory) boosting production of NAD+.
N-acetyl cysteine (NAC) to reduce oxidative stress, CRP (an inflammation marker), D-dimer (a clotting marker) and mucus production levels, although studies are not in agreement about how effective this is.
{kind=link}
More Ahead, Sometime
I am not sure when I will post Part 2 of this. I am gathering more information, especially watching someone who has been intensely methodical about her Long COVID for years and may have found a personal breakthrough.
But this post became somewhat urgent as more friends got in touch to say they have Long COVID or are in the midst of acute COVID now and want to know what they can do. (I now have to do some work I postponed to write this, so I may not post for Monday.)
It’s especially a pickle in the UK where the government is discarding Paxlovid doses it bought and didn’t administer, letting them expire instead, and discarding millions of doses of vaccine that it bought and didn’t allow people to get. That’s why my suggestions here include so many items people can buy without a prescription.
If you have access to prescription medications, pursue them. They are more effective than non-prescription substances. The earlier you get them, the more likely they are to help you, so please don’t put it off.
Also please remember, I am not a doctor or a biochemist. Look into everything I’ve suggested before you try it—you may decide I’m wrong about some of this, or may decide it’s simply not for you.
As always, Your Mileage May Vary. But if you’ve had COVID and need help with the consequences, I hope something here will be useful to you.
The next post in this series is After Getting COVID, Part 2.
Note: This post was edited 2024-06-18, primarily to add mention of a couple of substances.