


Make the Odds Be In Your Favor

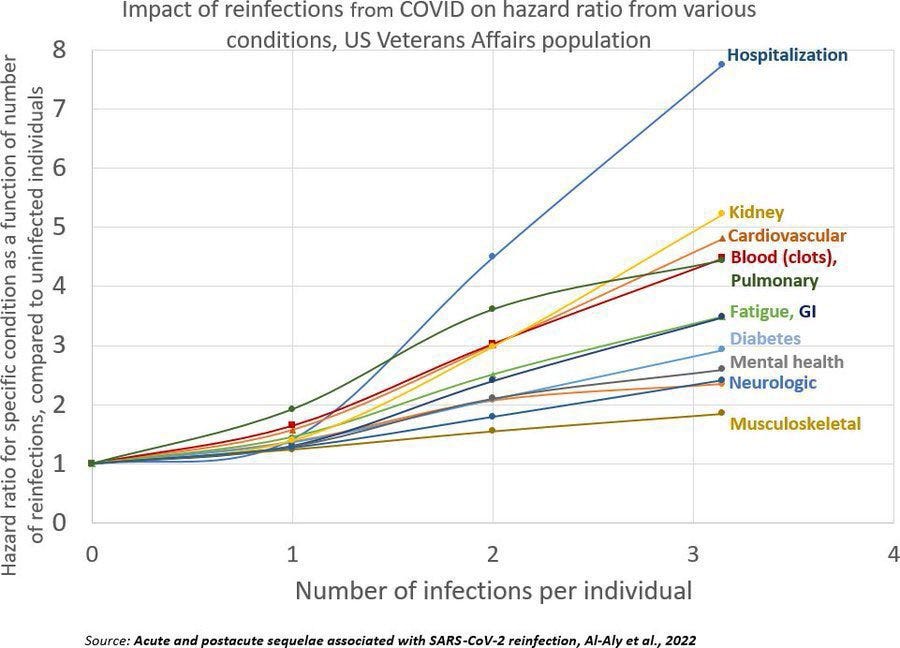
(Chart by @Wikisteff based on a study in Nature Medicine)
Please make sure you have a good supply of high quality face masks, at least N95 (FFP2), preferably N99 (FFP3). In a moment I’ll explain why. The chart of reinfection outcomes is only a piece of the picture.
Also check your stock of replacement filters for any HEPA filters or Corsi-Rosenthal boxes you have. If you don’t have enough face masks or filters to see you through to the warm season when people can visit outside with social distancing, stock up now.
Bear in mind that high quality masks will work until they start to show wear or start to not fit as snugly as they did at first. That can stretch your supply and your money considerably. The usual routine is to have three masks in service at a time. Use mask #1 and hang it up at the end of the day in a clean, dry, safe place to air out. The next day, use mask #2 and do the same. Ditto for mask #3. Then start the cycle again with mask #1. With this routine, you allow each mask to air out long enough for SARS virus on or in it to die before you use it again.
Why? Because of XBB.1.5.
Why Is This Flavor Different?
This subvariant appears to have arisen in New York. Genetically, it is almost as different from the original SARS2 (Wuhan) as SARS2 is from SARS1. We might as well be dealing with a new (SARS3) coronavirus.
Even our bivalent vaccines aren’t close enough to do a good job against this new subvariant. Most of the drugs we developed for treatment don’t work any more. Evusheld can’t protect the immunocompromised from it. Rapid home tests had a 47% false negative rate this past autumn and they are even less reliable at detecting this, often showing negative throughout a definite COVID case. Anecdotal reports suggest PCR tests can miss it too.
Most pandemic surveillance has been stopped or dismantled. We don’t know how severe it tends to be, how likely it is to leave survivors with Long COVID, etc. What we see happening to health care systems suggests it is not milder and instead is more severe. Data isn’t solid enough to quantify that statement. Looking at what is happening to major health care systems where this subvariant has arrived gives a sense that this is not like Omicron a year ago.
We know XBB.1.5 spreads like wildfire. Its R₀ is 10 to 18. That means each person who gets infected gives it to that many other people. That puts it in the same league with measles, which is famously contagious with a R₀ often cited as 12 to 18.
Recap of What People Shrug Off
In the past I’ve tried to get people to understand the initial illness is not the whole story. Today I’ve got another perspective for you, but here’s a quick recap of a few lowlights from what doesn’t matter to so many people.
On average, people have about a 40% higher chance of dying in the year after they “survive” COVID. That’s a full-spectrum average. The figures are higher in the elderly.
People under 65 years old with no prior risk factors who “recover” from COVID still have higher risks. Looking at only cardiovascular impact, in the year after even a ‘mild’ case of COVID, they are
52% more likely to have a stroke
63% more likely to have a heart attack
72% more likely to have heart failure
If you think those are treatable, you must not be one of my British readers. The average time for an ambulance to come for heart attack or stroke in England is supposed to be 18 minutes. Right now it is over 90 minutes. By the time an ambulance arrives, the Golden Hour is gone. (The first hour after a stroke or heart attack is when treatment options are best and have the highest chance of turning out well.) When we do reach the hospital, that doesn’t mean medical care will begin. Getting to the hospital is now, statistics say, the start of a much longer wait.
Back to aftermath… What about children, in whom some people claim COVID is no big deal? Kids are 72% more likely to develop Type 1 diabetes after a bout with the virus.
Many people look at all of that, shrug, and continue to mix with other people without taking precautions. Many people have swallowed the false narrative that having a bout with COVID leaves their immune system stronger. It’s inevitable, they say, and they’ll be better off each time they get it.
Really? Really not!
Reinfection Makes You More Vulnerable
Now look again at the chart of COVID outcomes from reinfection. The data is from a study in Nature Medicine with the title Acute and postacute sequelae associated with SARS-CoV-2 reinfection.
The chart makes it abundantly clear that you wouldn’t emerge from a bout of this disease with better resistance against it. You would emerge weaker. Each time you get it, you’re more likely to get sicker.
You’re more likely to stay sick, too. Reinfections increase the chance of ending up with Long COVID. If your first bout with COVID was "Moderate with Hospitalization," your chance of dying from a second COVID infection is not the common-wisdom 1%, it’s about 4%.
All of this argues for not waiting to hear officials say it’s time to take precautions now that we have a rip-roaring super contagious flavor of the virus circulating. By the time they say anything, it will be too late for too many people. I don’t want you to be among those people.
If you have gotten a little complacent in recent months, this would be a good time to revive some habits from earlier in the pandemic. If you are unwilling to do without indoor visits, at least run a hefty HEPA filter (or two) during visits. During the holidays, my wife inadvertently did a real-world test of our filter. She had someone over for dinner while I was away. They were indoors, unmasked, but sat across from each other in the living room (about 8 feet apart). The windows were only open a little bit. But our HEPA filter ran near my wife. The next morning my wife woke up with a bad cold she had caught from a different friend a few days earlier. (It really does seem to have been only a cold.)
The friend who came to dinner never came down with the cold. The filter and social distancing protected her.
Why Stock Up on Supplies?
The wave this subvariant is starting has already begun to disrupt factories. It’s in business news. When warehouses run low, they’ll have difficulty restocking. If you want masks, filters or anything else from a factory (in my case, replacing a couple of security lights that have failed, as an example), the time to get them is now.
XBB.1.5 looks like it will make a bigger impact than waves of other recent subvariants. So please revive your best pandemic-safe habits and make sure you have enough supplies on hand to ride out supply chain disruptions.
Make the odds be ever in your favor.
Well this is distressing. Mother Nature really wants us gone. Are your masks the paper-type ones? I didn't think those were meant to be reused after a day's use. This is the only supplier I could find of ffp3 masks in the US: https://www.ctbiotech.com/collections/n95-masks-and-respirators/products/andum-ffp3-respirator-with-headbands?variant=42328409407700
In light of this information, I'd like to ask if you'd explain something to me. You've mentioned previously that you eat/drink while wearing a mask, and I've done the same, but I currently use KN95s with ear loops; I grab a breath, unloop one side, eat or drink, then immediately replace the loop & mask.
N95s have the head bands, so would you briefly describe the process you use to eat, please?
There are no precautions used in my workplace and I'm the only one who masks; I usually sit in my car to eat, but I frequently drink water during the day and don't have the option to go outside to do so.
And I just thought of this: do you put the Day 1 mask in a paper bag or hang it outside? And regarding clothes: I'm still not sure about the clothes I wear & if they potentially carry the virus, so I generally put them on the balcony as soon as I change, and then wash my hands before petting my cat.
Thank you, Bonnie.